

Understanding Pressure Ulcers: Prevention and Treatment Introduction Pressure ulcers, also...
Read More

















The Impact of Poor Circulation on Wound Healing
The Impact of Poor Circulation on Wound Healing Introduction Proper...
Read More
What Are Chronic Wounds and How Are They Treated?
What Are Chronic Wounds and How Are They Treated? A...
Read More
Antibiotic Stewardship in Wound Care: Managing Resistant Infections – Outline
Antibiotic Stewardship in Wound Care: Managing Resistant Infections – Outline...
Read More
The Role of Blood Circulation in Wound Healing
The Role of Blood Circulation in Wound Healing Wound healing...
Read More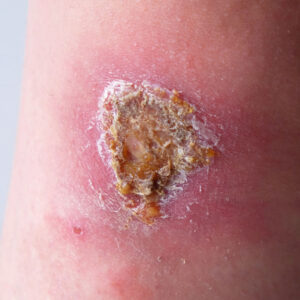
Signs of an Infected Wound
Signs of an Infected Wound Wound infections can turn a...
Read More
The Stages of Wound Healing Explained
The Stages of Wound Healing Explained Wound healing is a...
Read More
Acute vs. Chronic Wounds
Acute vs. Chronic Wounds: Understanding the Difference Wounds are an...
Read More