Congestive Heart Failure
Heart failure is a condition in which the heart can’t pump enough blood to meet the body’s needs. In some cases, the heart can’t fill with enough blood. In other cases, the heart can’t pump blood to the rest of the body with enough force. Some people have both problems.
The term “heart failure” doesn’t mean that your heart has stopped or is about to stop working. However, heart failure is a serious condition that requires medical care.

Overview
Heart failure develops over time as the heart’s pumping action grows weaker. The condition can affect the right side of the heart only, or it can affect both sides of the heart. Most cases involve both sides of the heart.
Right-side heart failure occurs if the heart can’t pump enough blood to the lungs to pick up oxygen. Left-side heart failure occurs if the heart can’t pump enough oxygen-rich blood to the rest of the body.
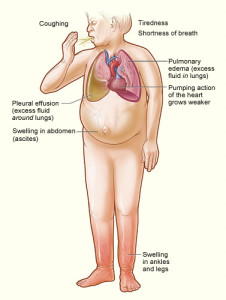
Right-side heart failure may cause fluid to build up in the feet, ankles, legs, liver, abdomen, and the veins in the neck. Right-side and left-side heart failure also may cause shortness of breath and fatigue (tiredness).
The leading causes of heart failure are diseases that damage the heart. These include coronary heart disease (CHD), also called coronary artery disease; high blood pressure; and diabetes.
Signs and Symptoms of Congestive Heart Failure
The most common signs and symptoms of heart failure are:
- Shortness of breath or trouble breathing
- Fatigue (tiredness)
- Swelling in the ankles, feet, legs, abdomen, and veins in the neck
All of these symptoms are the result of fluid buildup in your body. When symptoms start, you may feel tired and short of breath after routine physical effort, like climbing stairs.
As your heart grows weaker, symptoms get worse. You may begin to feel tired and short of breath after getting dressed or walking across the room. Some people have shortness of breath while lying flat.
Fluid buildup from heart failure also causes weight gain, frequent urination, and a cough that’s worse at night and when you’re lying down. This cough may be a sign of acute pulmonary edema (e-DE-ma). This is a condition in which too much fluid builds up in your lungs. Acute pulmonary edema requires emergency treatment.
Diagnosing Congestive Heart Failure
Your doctor will diagnose heart failure based on your medical and family histories, a physical exam, and the results of tests. Because the signs and symptoms of heart failure also are common in other conditions, your doctor will:
- Find out whether you have a disease or condition that can cause heart failure, such as coronary heart disease (CHD), high blood pressure, or diabetes
- Rule out other causes of your symptoms
- Find any damage to your heart and check how well your heart pumps blood
Early diagnosis and treatment can help people who have heart failure live longer, more active lives.
Medical and Family Histories
Your doctor will ask whether you or others in your family have or have had a disease or condition that can cause heart failure.
Your doctor also will ask about your symptoms. He or she will want to know which signs and symptoms you have, when they occur, how long you’ve had them, and how severe they are. Your answers will help show whether your symptoms limit your daily routine, and, if so, how much.
Physical Exam
During the physical exam, your doctor will:
- Listen to your heart for sounds that aren’t normal
- Listen to your lungs for the sounds of extra fluid buildup
- Look for swelling in your ankles, feet, legs, abdomen, and the veins in your neck
Diagnostic Tests
No single test can diagnose heart failure. If you have signs and symptoms of heart failure, your doctor may recommend one or more of the following tests. He or she also may refer you to a cardiologist. A cardiologist is a doctor who specializes in diagnosing and treating heart diseases and conditions.
EKG (Electrocardiogram)
An EKG is a simple, painless test that detects and records the heart’s electrical activity. The test shows how fast the heart is beating and its rhythm (steady or irregular). An EKG also records the strength and timing of electrical signals as they pass through each part of the heart.
An EKG may show whether the walls in your heart’s pumping chambers are thicker than normal. Thicker walls can make it harder for your heart to pump blood. An EKG also can show signs of a previous or current heart attack.
Chest X-Ray
A chest x-ray takes pictures of the organs and structures inside your chest, such as your heart, lungs, and blood vessels. This test can show whether your heart is enlarged, whether you have fluid in your lungs, or whether you have lung disease.
BNP Blood Test
This test checks the level of a hormone in your blood called BNP. The level of this hormone rises during heart failure.
Echocardiography
Echocardiography (echo) uses sound waves to create a moving picture of your heart. The test provides information about the size and shape of your heart and how well your heart chambers and valves are working.
Echo also can identify areas of poor blood flow to the heart, areas of the heart muscle that aren’t contracting normally, and previous injury to the heart muscle caused by lack of blood flow.
Echocardiography may be done before and after a stress test (see below). This is called a stress echo. A stress echo can show how well blood is flowing in various parts of your heart and/or how well your heart pumps blood when it beats.
Doppler Ultrasound
A Doppler ultrasound uses sound waves to measure the speed and direction of blood flow. This test often is done with echo to give a more complete picture of blood flow to the heart and lungs.
Doppler ultrasound often is used to find out whether you have right-sided heart failure (this is when the heart can’t fill with enough blood).
Holter Monitor
A Holter monitor records your heart’s electrical activity for a full 24- or 48-hour period, while you go about your normal routine.
You wear small patches called electrodes on your chest that are connected by wires to a small, portable recorder. The recorder can be clipped to a belt, kept in a pocket, or hung around your neck.
Nuclear Heart Scan
A nuclear heart scan shows how well blood is flowing through your heart and how much blood is reaching your heart muscle.
During a nuclear heart scan, a safe, radioactive substance called a tracer is injected into your bloodstream through a vein. The tracer travels to your heart and releases energy. Special cameras outside of your body detect the energy and use it to create pictures of your heart.
A nuclear heart scan can show where the heart muscle is healthy and where it’s damaged.
A positron emission tomography (PET) scan is a type of nuclear heart scan. It shows the level of chemical activity in areas of your heart. This test can help your doctor see whether enough blood is flowing to these areas.
A PET scan can show blood flow problems that other tests may not detect.
Cardiac Catheterization
During cardiac catheterization (KATH-e-ter-i-ZA-shun), a long, thin, flexible tube called a catheter is put into a blood vessel in your arm, groin (upper thigh), or neck and threaded to your heart. This allows your doctor to look inside your coronary (heart) arteries.
During this procedure, your doctor can check the pressure and blood flow in your heart chambers, collect blood samples, and use x rays to look at your coronary arteries.
Coronary Angiography
Coronary angiography (an-jee-OG-ra-fee) usually is done with cardiac catheterization. A dye that can be seen on an x-ray is injected into your bloodstream through the tip of the catheter.
The dye allows your doctor to see the flow of blood to your heart muscle. Angiography also shows how well your heart is pumping.
Stress Test
Some heart problems are easier to diagnose when your heart is working hard and beating fast. During stress testing, you exercise (or are given medicine if you can’t exercise) to make your heart work hard and beat fast. You may walk or run on a treadmill or pedal a bicycle.
Heart tests, such as nuclear heart scanning and echo, often are done during stress testing.
Cardiac MRI
Cardiac MRI (magnetic resonance imaging) uses radio waves, magnets, and a computer to create pictures of your heart as it’s beating. The test produces both still and moving images of your heart and major blood vessels.
A cardiac MRI can show whether parts of your heart are damaged. Doctors also use MRI in research studies to find early signs of heart failure, even before symptoms appear.
Thyroid Function Tests
Thyroid function tests show how well your thyroid gland is working. These tests include blood tests, imaging tests, and tests to stimulate the thyroid. Having too much or too little thyroid hormone in the blood can lead to heart failure.
Treatment Of Congestive Heart Failure
Early diagnosis and treatment can help people who have heart failure live longer, more active lives. Treatment for heart failure will depend on the type and stage of heart failure (the severity of the condition).
The goals of treatment for all stages of heart failure include:
- Treating the underlying cause of heart failure, such as coronary heart disease (CHD), high blood pressure, or diabetes
- Reducing symptoms
- Stopping the heart failure from getting worse
- Increasing your lifespan and improving your quality of life
Treatments usually include lifestyle changes, medicines, and ongoing care. If you have severe heart failure, you also may need medical procedures or surgery.
Lifestyle Changes
Simple changes can help you feel better and control heart failure. The sooner you make these changes, the better off you’ll likely be.
A Heart Healthy Diet
Following a heart-healthy diet is a crucial part of managing heart failure. In fact, not having a proper diet can make heart failure worse. Talk with your doctor and health care team to create an eating plan that works for you.
A heart-healthy diet includes a variety of fruits, vegetables, and whole grains. It also includes lean meats, poultry, fish, beans, and fat-free or low-fat milk or milk products. A healthy diet is low in saturated fat, trans fat, cholesterol, sodium (salt), and added sugar.

Too much salt can cause extra fluid to build up in your body, making heart failure worse. Saturated and trans fats can cause unhealthy blood cholesterol levels, which are a risk factor for heart disease.
A balanced diet with varied nutrients can help your heart work better. Getting enough potassium is essential for people who have heart failure. Some heart failure medicines deplete the potassium in your body. Lack of potassium may cause very rapid heart rhythms that can lead to sudden death.
Potassium is found in foods like white potatoes and sweet potatoes, greens (such as spinach), bananas, many dried fruits, and white beans and soybeans. Talk with your health care team about getting the correct amount of potassium.
For more information about following a healthy diet, see the National Heart, Lung, and Blood Institute’s Aim for a Healthy Weight Web site, “Your Guide to a Healthy Heart,” “Your Guide to Lowering Your Blood Pressure With DASH,” and “Your Guide to Lowering Cholesterol With TLC.” All of these resources include general information about healthy eating.
Proper Fluid Intake
It’s very important for people who have heart failure to drink the right amounts and types of fluid. Drinking too much fluid can worsen heart failure. Also, if you have heart failure, you shouldn’t drink alcohol.
Talk to your doctor about what amounts and types of fluid you should have each day.
Other Lifestyle Changes
Taking steps to control risk factors for CHD, high blood pressure, and diabetes also will help manage heart failure.
- Lose weight if you’re overweight or obese. Work with your health care team to lose weight safely.
- Do physical activity as your doctor directs to become more fit and stay as active as possible.
- Quit smoking, and avoid using illegal drugs. Talk to your doctor about programs and products that can help you quit smoking. Also, try to avoid secondhand smoke. Tobacco and drugs can worsen heart failure and harm your health.
- Get enough rest.
Medicines
Your doctor will prescribe medications based on the type of heart failure you have, how severe it is, and your response to certain medicines. The following medicines are commonly used to treat heart failure:
- Diuretics (water or fluid pills) help reduce fluid buildup in your lungs and swelling in your feet and ankles.
- ACE inhibitors lower blood pressure and reduce strain on your heart. They also may reduce the risk of a future heart attack.
- Aldosterone antagonists trigger the body to get rid of salt and water through urine. This lowers the volume of blood that the heart must pump.
- Angiotensin receptor blockers relax your blood vessels and lower blood pressure to decrease the workload on your heart.
- Beta blockers slow your heart rate and lower your blood pressure to decrease the workload on your heart.
- Isosorbide dinitrate/hydralazine hydrochloride helps relax your blood vessels, so your heart doesn’t work as hard to pump blood. The Food and Drug Administration approved this medicine for use in African Americans after studies showed it worked well for this group.
- Digoxin makes the heartbeat stronger and pump more blood.
Ongoing Care
It’s important to watch for signs that heart failure is getting worse. For example, weight gain may mean that fluids are building up in your body. Discuss with your doctor how often to check your weight and when to report weight changes.
It’s also important to get medical care for other related conditions. If you have diabetes and/or high blood pressure, work with your health care team to control these conditions. Have your blood sugar level and blood pressure checked. Talk with your doctor about when you should have tests and how often to take measurements at home.
Try to avoid respiratory infections like the flu and pneumonia. Talk with your doctor or nurse about getting flu and pneumonia vaccines.
Many people who have severe heart failure may need treatment in a hospital from time to time. Your doctor may recommend oxygen therapy (oxygen given through nasal prongs or a mask). Oxygen therapy can be given in a hospital or at home.
Medical Procedures and Surgery
As heart failure worsens, lifestyle changes and medicines may no longer control your symptoms. You may need a medical procedure or surgery.
If you have heart damage and severe heart failure symptoms, you may need a cardiac resynchronization therapy (CRT) device or an implantable cardioverter-defibrillator (ICD).
In heart failure, the right and left sides of the heart may no longer contract at the same time. This disrupts the heart’s pumping. To correct this problem, your doctor may implant a CRT device (a type of pacemaker) near your heart. This device helps both sides of your heart contract at the same time, which may decrease heart failure symptoms.
Some people who have heart failure have very rapid, irregular heartbeats. Without treatment, the problem can cause sudden cardiac arrest. Your doctor may implant an ICD near your heart to solve this problem. An ICD checks your heart rate and uses electrical pulses to correct irregular heart rhythms.
People who have severe heart failure symptoms at rest, despite other treatments, may need:
- A mechanical heart pump, such as a left ventricular assist device. This device helps pump blood from the heart to the rest of the body. You may use a heart pump until you have surgery or as a long-term treatment.
- Heart transplant. A heart transplant is an operation in which a person’s diseased heart is replaced with a healthy heart from a deceased donor. Heart transplants are done as a life-saving measure for end-stage heart failure when medical treatment and less drastic surgery have failed.
- Experimental treatments. Studies are underway to see whether open-heart surgery or angioplasty (a procedure used to open clogged heart arteries and improve blood flow) can reduce heart failure symptoms.
- Congestive heart failure (CHF) is a condition in which the heart’s function as a pump is now less than adequate to meet the needs of the body.
- Many disease processes can impair the pumping efficiency of the heart, which can cause congestive heart failure.
- The symptoms of congestive heart failure can vary with the individual patient, but these symptoms can include fatigue, diminished exercise capacity, shortness of breath, and swelling.
- The diagnosis of congestive heart failure is based on knowledge of the individual patient’s medical history, a careful physical examination, and selected laboratory tests.
- The treatment of congestive heart failure can include lifestyle modifications, addressing the potentially reversible factors, medications, a heart transplant, and even mechanical therapies.
The course of congestive heart failure in any given patient can vary greatly.
What is congestive heart failure?
Congestive heart failure (CHF) is a condition in which the heart’s function as a pump is no longer adequate to deliver oxygen-rich blood efficiently throughout the body. Congestive heart failure may be caused by:
- diseases that can weaken the heart muscle,
- diseases that can cause a stiffening of the heart muscles, or
- diseases that can increase the demand of oxygen by the body tissue beyond the capability that the heart has to deliver an adequate amount of oxygen-rich blood.
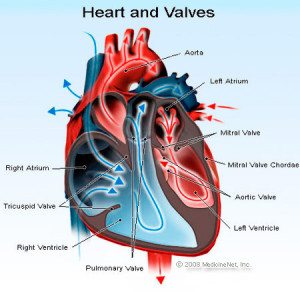
The heart has two atria (right atrium and left atrium) that make up the upper chambers of the heart, and the two lower chambers of the heart are made up of two ventricles (left ventricle and right ventricle). The ventricles are muscular chambers that pump blood when the muscles are contracted. The contraction of the ventricle muscles is known as asystole.
Many known diseases can impair the pumping action of these ventricles. For example, the muscles of the ventricles can be severely weakened by heart attacks, infections (myocarditis), or toxins such as alcohol and some chemotherapy agents. The diminished pumping ability of the ventricles due to muscle weakening is known as systolic dysfunction. After each ventricular contraction (systole), the ventricle muscles need to relax, which allows the blood from the atria to fill the ventricles. This relaxation of the ventricles is called a diastole.
Diseases such as hemochromatosis (iron overload) or amyloidosis can cause a stiffening of the heart muscle and can impair the ventricles’ capacity to relax properly and fill up; this is called a diastolic dysfunction. The most common cause of this is longstanding high blood pressure, which results in a thickening (hypertrophied) of the heart. Additionally, in some patients, although the pumping action and filling capacity of the heart may seem normal, abnormally high oxygen demand by the body’s tissues (for example, with hyperthyroidism or anemia) may make it extremely difficult for the heart to supply the adequate blood flow (called high output heart failure).
In some individuals, one or more of these factors may be present and be the cause of congestive heart failure. The remainder of this article will focus primarily on congestive heart failure that is due to the weakening of the heart muscle itself, systolic dysfunction.
Congestive heart failure can affect many of the organs of the body. Some examples are:
- Weakened heart muscles may not be able to properly supply the right amount of blood to the kidneys, which then can begin to lose their normal ability to excrete salt (sodium) and water. This diminished kidney function can cause the body to retain too much fluid.
- The lungs may even become congested with fluid (pulmonary edema) and the person’s ability to exercise is greatly decreased.
- Fluid can also accumulate in the liver, thereby impairing its functional ability to rid the body of toxins and produce essential proteins.
- The intestines may also become less efficient in absorbing nutrients and medicines.
- Fluid also may accumulate in the extremities, which results in edema (swelling) of the ankles and feet.
Eventually, untreated and worsening cases of congestive heart failure will affect virtually every organ in the body.
What are the major causes of congestive heart failure?
Many disease processes can impair the pumping efficiency of the heart and this is the cause of congestive heart failure. In the United States, the most common causes of congestive heart failure are as follows:
- coronary artery disease
- high blood pressure (hypertension)
- longstanding alcohol abuse
- disorders of the heart valves
- unknown (idiopathic) causes, such as after recovery from myocarditis
Some of the less common causes include viral infections for the stiffening of the heart muscle, thyroid disorders, disorders of the heart rhythm, and many others.
It should also be noted, that in some patients with underlying heart disease, taking certain medications can lead to the development or worsening of congestive heart failure. This is especially true for those drugs that can cause sodium retention or affect the strength and power of the heart muscle. Examples of some of these medications are the commonly used nonsteroidal anti-inflammatory drugs (NSAIDs), which include ibuprofen (Motrin and others) and naproxen (Aleve and others) as well as certain steroids, some medication for diabetes (such as rosiglitazone [Avandia] or pioglitazone [Actos]), and some calcium channel blockers.
What are some of the Symptoms of Congestive Heart Failure (CHF)?
The symptoms of congestive heart failure vary greatly among individuals according to the particular organ systems that are involved and depending on the degree to which the rest of the body has “compensated” for the weakening of the heart muscle.
- An early warning sign (symptom) of congestive heart failure is fatigue. While fatigue is a sensitive indicator of the possibility of underlying congestive heart failure, it is obviously a non-specific symptom that may be caused by many other possible conditions. The person’s ability to exercise may also be diminished. Patients may not even sense this decrease, and they may subconsciously reduce their activities in order to accommodate these limitations.
- As the body becomes overloaded with fluids from congestive heart failure, swelling (edema) of the ankles and legs or abdomen may be noticeable. This can be referred to as “right-sided heart failure” as failure of the right-sided heart chambers to efficiently pump venous blood to the lungs to acquire oxygen results in a buildup of this fluid in gravity-dependent areas such as the legs. The most common cause of this is the longstanding failure of the left heart, which may lead to the secondary failure of the right heart. Right-sided heart failure can also be caused by severe lung disease (referred to as “cor pulmonale”), or by an intrinsic disease affecting the right heart muscle (less common).
- In addition, fluid may accumulate in the lungs, thereby causing breathing difficulties , particularly during exercise and when lying flat. In some instances, patients are awakened at night, gasping for air.
- Some patients may be unable to sleep unless sitting upright.
- The extra fluids building up in the body may cause increased urination, particularly at night.
- Accumulation of fluids in the liver and intestines may cause nausea, abdominal pain, and a decreased appetite.
How can congestive heart failure be diagnosed?
The diagnosis of congestive heart failure is most often a clinical one that is based on knowledge of the patient’s relevant medical history, a careful physical examination, and selected laboratory tests.
A thorough patient history may disclose the presence of one or more of the symptoms of congestive heart failure that were described above. In addition, a history of significant coronary artery disease, prior heart attack, hypertension, diabetes, or significant alcohol use can be major clues.
The physical examination is focused on detecting the presence of any extra fluids found in the body (breath sounds, leg swelling, or neck veins) as well as carefully characterizing the condition of the heart itself (pulse, heart size, heart sounds, and murmurs).
Useful diagnostic tests such as the electrocardiogram (ECG) and chest X-ray to detect previous heart attacks, arrhythmia, heart enlargement, and fluid in and around the lungs. One of the single most useful diagnostic test is the echocardiogram, which uses ultrasound to image the heart muscle, valve structures, and blood flow patterns. The echocardiogram is extremely helpful in diagnosing heart muscle weakness. In addition, the test can suggest possible causes for the weakening of the heart muscle (for example, prior heart attack, and severe valve abnormalities). Virtually all patients in whom the diagnosis of congestive heart failure is suspected should ideally undergo echocardiography as early as possible in their physical assessment.
Nuclear medicine studies assess the overall pumping efficiency of the heart and examine the possibility of inadequate blood flow to the heart muscle. Heart catheterization allows the arteries to the heart to be visualized with angiography (using dye inside of the blood vessels that can be seen using a chest X-ray). During catheterization, the pressures in and around the heart can be measured, and the heart’s performance properly assessed. In rare cases, a biopsy of the heart tissue may be recommended to diagnose specific diseases. This biopsy can often be accomplished through the use of a special catheter device that is inserted into a vein and be maneuvered into the right side of the heart.
Another very helpful diagnostic test is a blood test called a BNP or B-type natriuretic peptide level. The levels found in this form of testing can vary with age and gender but is typically elevated from heart failure and can aid in the diagnosis, and can be very useful in following the response to treatment of congestive heart failure.
The choice of tests depends on each patient’s individual case and is based on the suspected diagnoses.
What are the treatments for congestive heart failure?
Lifestyle Modifications
After congestive heart failure is diagnosed, treatment needs to be started immediately. Probably the most important and yet often most neglected aspect of treatment involves lifestyle modifications. Sodium has been proven to cause an increase in fluid accumulation in the body’s tissues. Because the body is often congested with excess fluid, patients become very sensitive to the levels of sodium and water intake. Restricting the intake of salt and fluid is often recommended because of the tendency of fluid to accumulate in the lungs and surrounding tissues. An American “no salt added” diet can still contain 4 to 6 grams (4000 to 6000 milligrams) of sodium daily. In individuals with congestive heart failure, an intake of no more than 2 grams (2000 milligrams) of sodium per day is highly advised. Reading food labels and paying very close attention to total sodium intake is critically important. Severe restriction of alcohol consumption also is strongly recommended.

Also, the total amount of fluids consumed must be regulated. Although many people with congestive heart failure take diuretics to aid in the elimination of excess fluid, the action of these medications can be overwhelmed by an excess intake of water and any other fluids. The maxim that “drinking eight glasses of water a day is healthy” definitely does not apply to patients with congestive heart failure. In fact, patients who show a more advanced cases of congestive heart failure are often advised to limit their total daily fluid intake from all sources to only 2 quarts. The above guidelines for sodium and fluid intake may vary greatly depending on the severity of congestive heart failure in any given individual patient and should be discussed at length with their physician.
An important tool for monitoring an appropriate fluid balance is the frequent measurement of individual body weight. An early sign of fluid accumulation is an increase in overall body weight. This may occur even before shortness of breath or swelling in the legs and other body tissues (edema) symptoms are detected. A weight gain of 2 to 3 pounds over 2 to 3 days should prompt an immediate call to the physician, who may order an increase in the dose of diuretics or other methods designed to stop the early stages of fluid accumulation before it can become more severe.
Aerobic exercise, once discouraged for congestive heart failure patients, has recently been shown to actually be beneficial in maintaining overall functional capacity, quality of life, and perhaps even improving patient survival. Each person’s body has its own unique ability to compensate for a failing heart. Even given the same degree of heart muscle weakness, individual patients may display widely varying degrees of limitation of function. Regular exercise, when tailored to each person’s tolerance level, appears to provide significant benefits and should be used only when the individual is compensated and stable.
Addressing the potentially reversible factors
Depending on the underlying cause of congestive heart failure, potentially reversible factors should definitely be explored. Some examples are:
- In certain persons whose congestive heart failure is caused by inadequate blood flow to their heart muscle, restoration of the blood flow through coronary artery surgery or catheter procedures (angioplasty, intracoronary stenting) may be considered.
- Congestive heart failure that is due to severe disease of the valves may be alleviated by valve surgery in certain appropriate patients.
- When congestive heart failure is caused by chronic, uncontrolled high blood pressure (hypertension), aggressive blood pressure control will often improve this condition.
- Heart muscle weakness that is due to longstanding, severe alcohol abuse can improve significantly with abstinence from drinking any alcohol.
- Congestive heart failure that is caused by other disease states may be similarly partially or wholly reversible with appropriate measures.